AUTOTRANSFUSION EQUIPMENT
WORLD FIRST TECHNOLOGY IN A SINGLE EQUIPMENT FOR YOUR SURGERY - SAVE YOUR BLOOD, SAVE YOUR LIFE.
THE BEST BLOOD A PATIENT CAN RECEIVE IS HIS OWN BLOOD.
CELL-SAVER XTRA Blood Recovery Pre, Intra and Postoperative
Sensors: double hematocrit, red blood cells, quality, air bubble, emptying and fluid
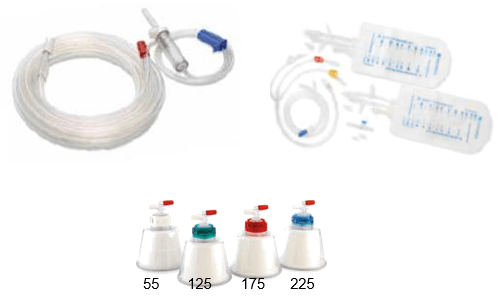
03 Tamnhos de Bowl 55, 125, 225 mL
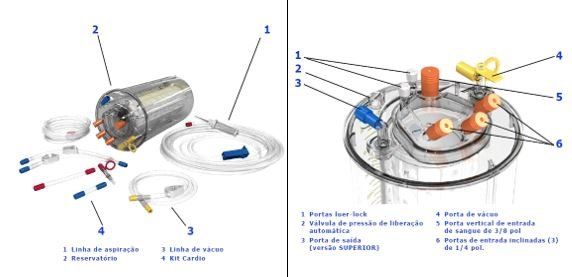
Reservoir with Filter of 40 µm micrometers
Blood Kit (ATS) and Plasma and Platelet Kit (Sequestration)
5,600 rpm centrifuge, silent vacuum pump, usb, LCD screen
Recovery rate 90%
medical protocols installed on the machine (POPT, PSTD, PFAT, POST-OP, EMERGENCY, PPP, PRP1, PRP2, RETURN, CONCENTRATE, REMOVAL, FILL IV
Operation and its functions, technical details

XTRA has a device for direct connection of the ATS (blood) equipment to the (Extracorporeal) CEC and post-op vacuum mode
XTRA is the sixth generation of autotransfusion equipment, compare with previous ELECTA equipment


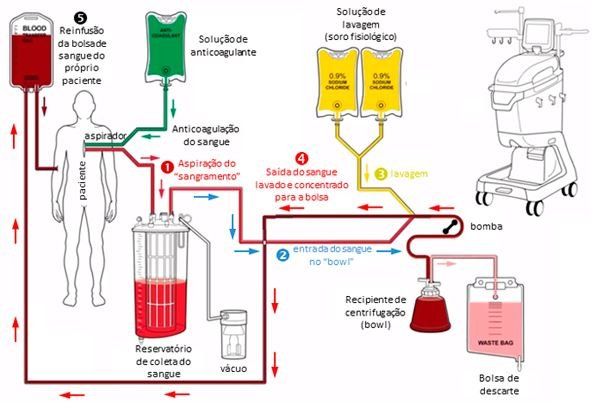
The XTRA equipment produced by Livanova is automated to return blood with extreme quality. Its German engineering transforms the product today into the best in the world, with very balanced rates in its final result (washed red blood cells returned to the patient). There are 4 processing cycles with the blood
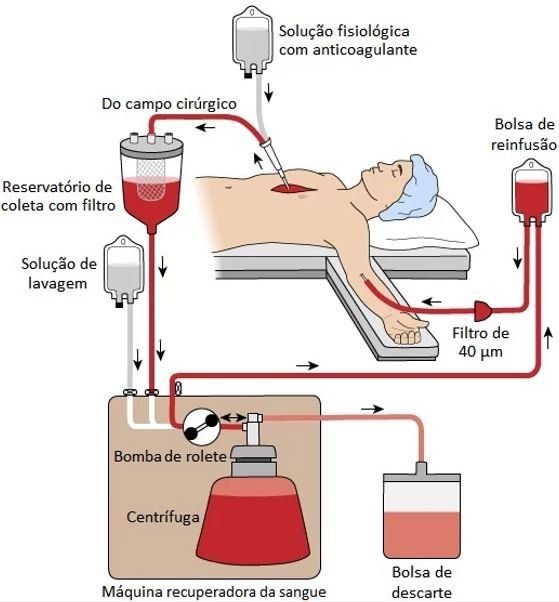
Aspiration: blood is aspirated from the surgical field, simultaneously mixed with the anticoagulant solution and temporarily stored in the reservoir.
Continuous and independent step, it is aspirated directly from the surgical field, using: use of heparin solution (1000mL of 0.9% saline solution + 5.0 mL of heparin = 25,000 UI);
Collected from the Extracorporeal Circuit (cardio kit)
Vacuum pressure (for hemolysis control): -100mmHg to -150mmH
The reservoir has a 40 µm filter - removes fat, tissue remains including bone and other particles larger than 40 µm;
Wet the filter with up to 200mL of the anticoagulant solution only after turning on the vacuum.
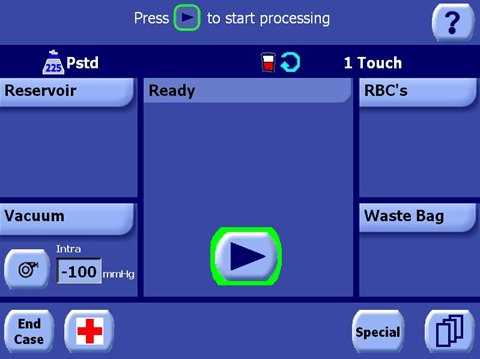
Possibility of manual start at any time, pressing the "start" key (play) in the center of the main menu
Filling / Prime : the blood is pumped from the reservoir to the hermetically produced bowl so as not to hemolyze the cells that arrive at the rotation speed of 5600rpm. The blood components are separated, the red cells are concentrated and the supernatant is discarded.
Automatic start by programming the scale volume
Wash / Wash : the blood is pumped from the reservoir to the bowl which arrives at a rotation speed of 5600rpm. The blood components are separated, the red cells are concentrated and the supernatant is discarded.
Wash red blood cells with a predetermined volume of saline
(different for each bowl);
Removes free hemoglobin in plasma, cell stroma, clotting factors, heparin and medications that do not bind to red blood cells.
Sensor indicates when washing is satisfactory (can interrupt the cycle if necessary);
In “Popt” adjust the washing flow to 300 ml/min
At this stage 100% of the heparin is discarded
Emptying: sending the washed red blood cell concentrate from the bowl (htc between 50% and 65%) to the reinfusion bag.
According to the manufacturer, the hematocrit of the CH obtained varies between 50% and 70% depending on the parameters used during the procedure.
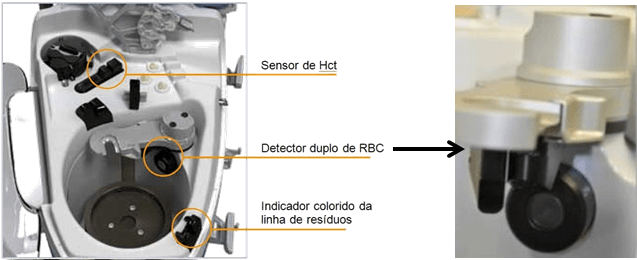
The equipment has 02 hematocrit sensors



ONE SYSTEM FOR ALL SURGERY AND PATIENTS
The XTRA system is very complete, automatic, innovative, promoting with its installed protocols:
Intraoperative Autotransfusion - ''Ats'' Popt, Pstd, Pfat, Purg
Postoperative Recovery - Post-op
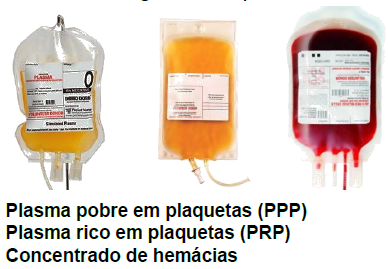
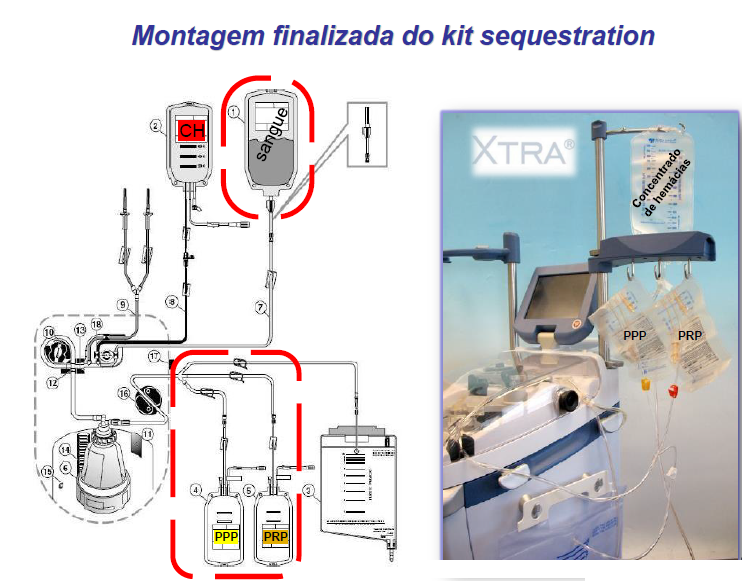
Preoperative apheresis - "Sequestration'' Separation of red blood cells, plasma and PPP/PRP platelets into separate pouches for use at any time during surgery
SPECIAL FUNCTIONS
Return: sends the blood from the bowl back to the reservoir;
Concentrate: “pulls” blood from the reinfusion bag into the bowl (used to fill a partially filled bowl);
Removal: removes air from the bag before reinfusion (prevents embolism);
Fill IV: function that sends (wash) serum to the reinfusion bag. Used in JEHOVAH'S WITNESSES surgeries where the ATS circuit must have continuity with the patient.






QUALITY AND SAFETY SENSORS
8.4“ “fullcolor” LCD screen with large viewing area and touch-sensitive;
A single “physical” button: STOP function;
Modular information: subfolders open and close with a simple
Touch;
All menus in PORTUGUESE, easy and intuitive
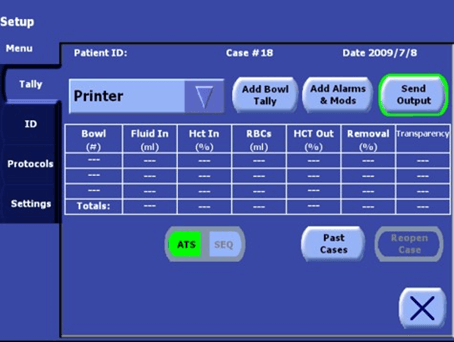
Screen with compiled data sheets and allows access to past cases
Stores up to 10,000 cases
USB ports for simultaneous transfer of multiple cases
integrated printer
RS232 ports for service and new functions under development
Dual sensor for red blood cell level detection. 02 optical sensors that allow a better filling of the bowl = higher final HTC and better washing
Integrated hematocrit sensor (optical sensor)
Wash quality sensor (discard line color)
air bubble sensor
Discard bag level (software)
Drain line sensor (reinfusion)
Centrifuge fluid loss sensor
Powerful and silent vacuum module, integrated into the XTRA user interface. however it can also be used separately as a vacuum module


DISPOSABLE PROCEDURE KITS THAT ARE INSTALLED ON THE EQUIPMENT
ATS E SEQUESTRATION
ATS (Sangue)
contains all components necessary for blood collection and processing
Suction and anticoagulation items, Blood collection reservoir,
Wash Kit with new bowl fitting and simplified cartridge design for easier and faster installation and
better performance
Higher Hcts and faster processing;
Color mount code
(blue, yellow, orange and white);
Automatic docking and undocking of the line in the peristaltic pump;
Automatic bowl size detection.
There are 03 types of bowl, to guarantee greater flexibility to face any operational situation
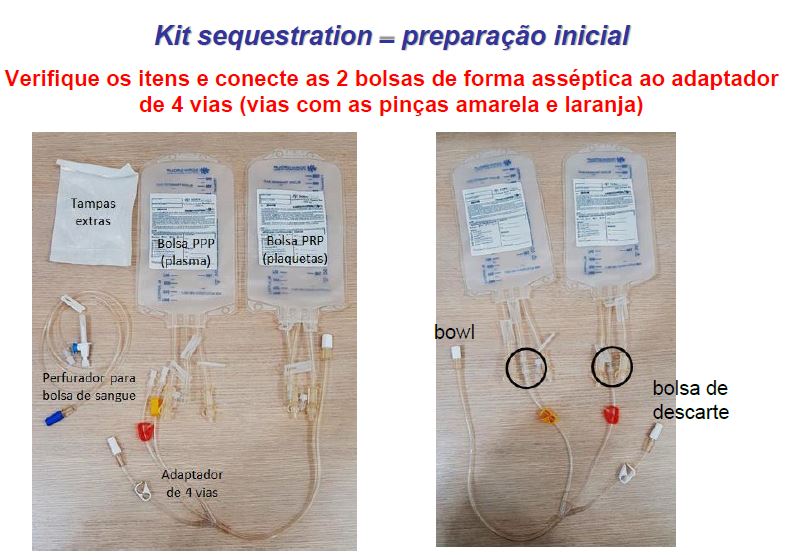
SEQUESTRATION (Plasma and Platelet)
Performed in the perioperative period
Evolution of hemodilution
Collect the patient's whole blood in a citrate bag
Processing on equipment with specific PPP/PRP protocol
Preserve plasma and platelets in different bags and also the red blood cells for reinfusion when necessary
PRP can be used to prepare platelet gels to be applied to tissue to improve regeneration.



SEQUESTRATION - PERIOPERATORY APHERISIS
Different procedures can be performed during the perioperative period with the same equipment
cell savior.
Preoperative collection of blood components (PPP, PRP); Blood recovery; Intraoperative Processing of stored allogeneic blood (blood bags); Postoperative blood recovery.
Perioperative apheresis : Advancement of acute normovolemic hemodilution ; By centrifuging the blood
total preserves autologous blood components separately Poor plasma

QUANTITY OF HEMOCOMPONENTS OBTAINED IN THE PROCEDURE
Platelet concentrate) CP (can be obtained from individual units of whole blood or by apheresis, collected from a single donor. Each unit of CP contains approximately 5.5 x 10 10 platelets in 50 - 60 mL of plasma, whereas the units per apheresis contains at least 3.0 x 1011 platelets in 200 - 300 mL of plasma (corresponding to 6 to 8 CP units per unit)
HOW IS THE SEPARATION IN DIFFERENTIATED CENTRIGUATION DONE?
Filling (PRIME)
Similar to the PRIME of intraoperative recovery: filling the bowl with concentration of red blood cells and sending the PPP to the collection bag (leave the yellow clamp open). Spillover (SPILL) The centrifuge decelerates to 2400RPM to unpack the Buffy-coat where the RBCs are.
The pump continues to fill the bowl and the PRP is directed to another bag (close the yellow clamp and open the orange clamp).
Emptying (EMPTY)
After the PRP overflows, the centrifuge stops spinning and the red blood cells are sent to the reinfusion bag.


COMMON QUESTIONS
- Does recovered blood contain heparin? NOT. Heparin is removed during washing as it concentrates in the same plasma phase after centrifugation. If you don't have heparin, why does the activated clotting test (ACT) give an incoagulable result? This is because clotting factors and platelets are not present in the recovered blood. Without it, the blood does not clot; and not by the presence of heparin. When I reinfuse the recovered blood, I observe worsening in the patient's clotting. Why? This can occur in cases of high processed volume. Only red blood cells are reinfused, as platelets and clotting factors are discarded. The worsening of the patient's clotting can be explained by a dilutional thrombocytopenia.
How soon should the recovered blood be reinfused into the patient? The reinfusion bag must be kept at room temperature and reinfused into the patient within 4 hours. It is recommended to carry out reinfusion while still in the operating room, in order to avoid the risk of transfusion in another patient.
Videos demonstrating the XTRA and its assembly with the KIT
XTRA
The XTRA Autotransfusion System is the complete solution for blood usage management and patient neurological protection. offers red blood cells
washed, fresh and viable autologous cells, significantly decreasing the inflammatory response and reducing the risks related to homologous blood transfusion.
LivaNova XTRA, in addition to reducing the inflammatory risk, also reduces the risk of fat embolism®, thanks to the new Pfat operating protocol that removes more than 99% of fat particles from processed blood intra or postoperatively?

References
1. Ashworth A, Klein AA. Br J. Cell salvage as part of a blood conservation strategy in anaesthesia. Anaesth. 2010 Oct;105(4):401-16. Epub 2010 Aug 28.2. Overdevest EP, Lanen PWJ, Feron JCM, van Hees JWH, Tan MESH. Clinical evaluation of the Sorin Xtra® autotransfusion system. Perfusion. 2012 Jul; 27(4):278–283. / 3. Shantikumar S, PatelS, Handa A.The role of cell salvage autotransfusion in abdominal aortic aneurysm surgery. Eur J Vasc Endovasc Surg. 2011 Nov; 42(5):577-84. Epub 2011 Jun 25.4. Kuppurao L, Wee M. Perioperative cell salvage. Contin Educ Anaesth Crit Care Pain. 2010; 10(4):104-108.5. Gäbel J, Westerberg M, Bengtsson A, Jeppsson A. Cell salvage of cardiotomy suction bloodimproves the balance between pro- and anti-inflammatory cytokines after cardiac surgery. Eur JCardiothorac Surg. 2013 Sep;44(3):506-11.6. Dabrowski W, Rzecki Z, Pilat J, Czajkowski M. Brain damage in cardiac surgery patients. Curr Opin Pharmacol. 2012 Apr;12(2):189-94. Epub 2012 Feb 9.7. Seyfried TF, Gruber M, Breu A, Aumeier C, Zech N, Hansen E. - Fat removal during cell salvage: an optimized program for a discontinuous autotransfusion device - Transfusion. August 2015 -Epub ahead of print.